Fractures of the pedal bone can be diagnosed in horses of all ages, including foals. They are typically caused by acute trauma e.g. a kick to a hard, immoveable object. Fast work is also capable of inducing fracture of the pedal bone. The forelimb is more commonly affected than the hindlimb.
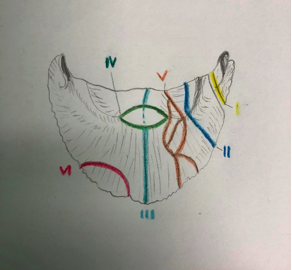
There are 6 classifications of pedal bone fracture (see diagram):
- Abaxial or paramedian (‘wing’) fractures without joint involvement (type I)
- Abaxial or paramedian (‘wing’) fractures with joint involvement (type II)
- Axial/sagittal and perisagittal fractures with joint involvement (type III)
- Fractures of the extensor process (type IV)
- Multifragment (comminuted) fractures with joint involvement (type V)
- Solar margin fractures (type VI)
Clinical Signs and Diagnosis
Affected horses will show an acute onset, moderate to severe lameness, which may be worse on turns. There is typically heat on palpation of the hoof and distal limb with an increased digital pulse. Hoof tester pain is common. Where there is involvement of the coffin joint, arthrocentesis may yield blood tinged synovial fluid. Nerve blocking of the foot should resolve the lameness. A hoof abscess is a differential diagnosis. X-rays are used to confirm the diagnosis in most cases. Multiple x-rays taken from different angles are required. In the very early stages, a fracture with minimal displacement will appear like a hairline and can be difficult to detect, repeat x-rays after 7-10 days of box rest may be necessary. With time, there is lysis of bone along the fracture line and a ‘fracture gap’ becomes more prominent, aiding radiographic detection. Complex and obscure cases may be imaged using scintigraphy, CT or MRI to give the best information regarding treatment, rehabilitation and prognosis for recovery.
Treatment
Foals are often managed with box rest. In mature horses, fractures of the pedal bone can be treated with fragment removal, cast application, special shoeing or surgery – depending on the nature of the injury.
Type I and II
These fractures respond best to a cast or a bar shoe with side clips. If there is significant displacement a surgical screw may be placed. Anti-inflammatory medication helps to relieve discomfort and enable weight bearing. Rest for 2-4 months is required, with follow up radiographs guiding assessment of fracture healing. Exercise is typically resumed at 4 months post injury. A reasonable prognosis for future use applies.
Type III
These fractures bisect the pedal bone. Conservative treatment options as described above apply. Surgical screws are also used. However, the rest period is far more prolonged. 4 months rest is followed by 4 months walking exercise. Surgically treated horses carry a better prognosis for return to exercise than those conservatively managed.
Type IV
These fragments can occur via 3 known mechanisms: hyperextension injury, avulsion by the extensor tendon and a separate centre of ossification. Horses may not exhibit any clinical signs and the fragment may be found incidentally during radiographs. Small fragments should be removed via arthroscopy. There is no ideal treatment for large fragments.
Type V
Comminuted fractures are associated with severe lameness. Application of a fibreglass cast may be attempted; however, these fractures carry a poor prognosis for future soundness. Euthanasia must be contemplated. A neurectomy may be performed is euthanasia is not an option.
Type VI
Solar margin fractures occur often and are underdiagnosed. They can develop as a result of trauma, but can also develop as a result of chronic laminitis.
Type VII
These are marginal fractures specific to foals.
Prepared with reference to FEI Campus materials